


Cardiac Imaging
Cardiac Imaging
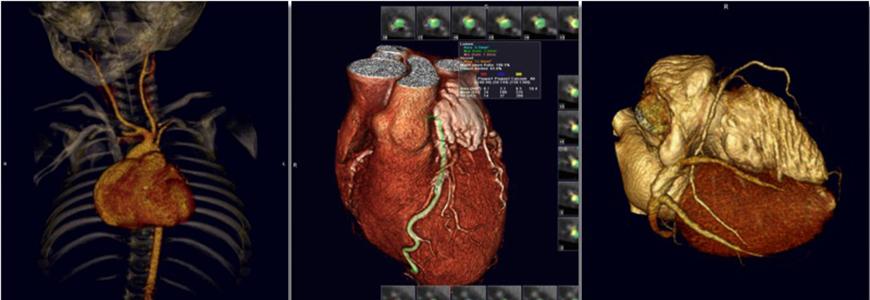
Clinical non-invasive cardiac imaging services, using the latest magnetic resonance imaging (MRI) and computed tomography (CT) technologies are used to diagnose a variety of heart conditions.
Both cardiac MRI and CT can be used to provide high quality cross-sectional images of the heart and the great vessels, in any desired orientation. Both modalities are useful for evaluating anatomic cardiac abnormalities, such as cardiac masses or congenital heart disease.
MRI additionally provides excellent dynamic and quantitative information on cardiac function and on large vessel and cardiac chamber blood flow. MRI is also very effective for detection of scarring of the heart wall, which can be valuable in the evaluation of myocardial viability for planning the treatment of coronary artery disease. CT provides better images of the coronary arteries than MRI, and it can be very helpful in detecting and characterizing atherosclerotic coronary artery disease as well as for evaluating coronary anomalies.
“ There are many different imaging tools for the heart. The development of cardiac imaging has made a real difference in the lives of many patients.”

CT Angiography - What is CT Angiography?
- CT (computed tomography) angiography (CTA) is an examination that uses x-rays to visualize blood flow in arterial vessels throughout the body, from arteries serving the brain to those bringing blood to the lungs, kidneys, and arms and legs.
- CT combines the use of x-rays with computerized analysis of the images.
- Beams of x-rays are passed from a rotating device through the area of interest in the patient’s body from several different angles so as to create cross-sectional images, which then are assembled by computer into a three-dimensional picture of the area being studied.
- Compared to catheter angiography, which involves placing a catheter and injecting contrast material into an artery, CTA is a much less invasive and more patient-friendly procedure-contrast material is injected into a peripheral vein rather than an artery.
- This exam has been used to screen large numbers of individuals for arterial disease. Most patients have CT angiography without being admitted to a hospital.
What are some common uses of the procedure?
- Examine the pulmonary arteries in the lungs to rule out pulmonary embolism, a serious but treatable condition.
- Visualize blood flow in the renal arteries (those supplying the kidneys) in patients with high blood pressure and those suspected of having kidney disorders. Narrowing (stenosis) of a renal artery is a cause of high blood pressure (hypertension) in some patients, and can be corrected. A special computerized method of viewing the images makes CT renal angiography a very accurate examination. Also done in prospective kidney donors.
- Identify aneurysms in the aorta or in other major blood vessels. Aneurysms are diseased areas of a weakened blood vessel wall that bulges out-like a bulge in a tire. Aneurysms are life-threatening because they can rupture.
- Identify dissection in the aorta or its major branches. Dissection means that the layers of the artery wall peel away from each other-like the layers of an onion. Dissection can cause pain and can be life-threatening.
- Identify a small aneurysm or arterio-venous malformation inside the brain that can be life-threatening.
- Detect atherosclerotic disease that has narrowed the arteries to the legs.
- CTA also is used to detect narrowing or obstruction of arteries in the pelvis and in the carotid arteries bringing blood from the heart to the brain.
- When a stent has been placed to restore blood flow in a diseased artery, CT angiography will show whether it is serving its purpose. Examining arteries in the brain may help reach a correct diagnosis in patients who complain of headaches, dizziness, ringing in the ears, or fainting.
- Injured patients may benefit from CTA if there is a possibility that one or more arteries have been damaged. In patients with a tumor it may be helpful for the surgeon to know the details of arteries feeding the growth.
How should I prepare for the procedure?
- Patients should be encouraged to drink fluids the evening before or the morning of the procedure to ensure they are well hydrated prior to the study.
- Depending on the part of the body to be examined, you may be asked to take only clear liquids by mouth before CTA.
- You will be asked whether you have asthma or any allergies to foods or drugs, and what medications you are currently taking. If you are pregnant, you should inform the technologist before the procedure.
- You probably will not have to undress if you are having an exam of the head, neck, arms or legs.
- Remove any jewellery, hair clips, dentures and the like that could show up on the x-rays and make them hard to interpret.
What does the equipment look like?
- A CT scanner is a specialized x-ray machine that looks like a large doughnut. It has an opening measuring about two feet in diameter that surrounds a narrow table.
- Inside the frame of the scanner is a rotating device with an x-ray tube mounted on one side and a banana-shaped detector opposite it.
- Many CTA studies use an advanced type of unit called a spiral CT machine that looks like any other type of CT unit, but is able to record a large number of pictures in a short time. This means that patients do not have to hold their breath for a prolonged period.
How does the procedure work?
- Before the actual exam begins, the patient will have a dose of contrast material injected into a vein to make the blood vessels stand out.
- An automatic injector machine is used that controls the timing and rate of injection, which may continue during part of the time images are recorded.
- During the examination, the rotating device spins around the patient, creating a fan-shaped beam of x-rays, and the detector takes snapshots of the beam after it passes through the patient.
- As many as one thousand of these pictures may be recorded in one turn of the detector.
- The real work of CTA comes after the images are acquired, when powerful computer programs process the images and make it possible to display them in different ways, for instance, in cross-sectional slices or as three-dimensional “casts” of the blood vessels.
- A radiologist, a medical doctor specializing in CT Angiography interprets the images to make a diagnosis and prepare a report for the referring physician.
What will I experience during the procedure?
- CTA takes about 10 to 25 minutes from the time the actual examination begins.
- Overall, you can expect to be in or near the examining room for 20 to 60 minutes.
- You may feel warm all over when contrast material is injected before the scan, but you should not feel pain at any time.
- Any CT study requires that you remain still during the exam. Pillows and foam pads may help make it more comfortable. At the same time the nurse or technologist may use pads or Velcro straps to keep the area from moving.
- The examination table will move into and out of the scanner opening, but it is not enclosed and only a small part of your body will be inside at any one time.
- You may be asked to hold your breath for 10 to 25 seconds to be sure that the images will not be blurred.
- During the time that no actual imaging is taking place you are free to ask questions or talk to the technologist, but friends or relatives will not be allowed in the examining room.
- Once the needed images have been recorded, you will be free to leave.
- You can eat immediately and it is a good idea to drink plenty of fluids in the hours after the exam to help flush contrast material out of the system.
Who interprets the results and how do I get them?
- Typically the results of CTA are available within 24 hours, although in complicated cases special computer analysis may take somewhat longer.
- The radiologist will report the findings to your physician, who in turn will discuss them with you.
What are the benefits vs. risks?
Benefits
- CTA can be used to examine blood vessels in many key areas of the body, including the brain, kidneys, pelvis, and the arteries serving the lungs. The procedure is able to detect narrowing of arteries in time for corrective surgery to be done.
- This method displays the anatomical detail of blood vessels more precisely than magnetic resonance imaging (MRI) or ultrasound. Today many patients can have CTA in place of a conventional catheter angiogram.
- CTA is a useful way of screening for arterial disease because it is safer and much less time-consuming than catheter angiography and is a cost-effective procedure. There also is less discomfort because contrast material is injected into an arm vein rather than into a large artery in the groin.
Risks
- There is a risk of an allergic reaction-which may be serious-whenever contrast material containing iodine is injected. If you have a history of allergy to x-ray dye, your radiologist may advise that you take special medication for 24 hours before CTA to lessen the risk of allergic reaction. Another option is to undergo a different exam that does not call for contrast injection.
- CTA should be avoided in patients with kidney disease or severe diabetes because x-ray contrast material can further harm kidney function.
- If a large amount of x-ray contrast leaks out under the skin where the IV is placed, skin damage can result. If you feel any pain in this area during contrast injection, you should immediately inform the technologist. Women should always inform their doctor or x-ray technologist if there is any possibility that they are pregnant.
What are the limitations of CT Angiography?
- CTA images of blood vessels anywhere in the body may be fuzzy if the patient moves during the exam or if the heart is not functioning normally.
- Blocked blood vessels also may make the images hard to interpret. CTA is not yet able to reliably image small, twisted arteries or vessels in organs that move rapidly.
- If you are breast-feeding at the time of the exam you should ask your radiologist how to proceed. It may help to pump breast milk ahead of time and keep it on hand for use after CTA contrast material has cleared from your body.
- Pregnant women, especially those in the first three months, should not have CTA or any exam exposing them to x-rays.
MR Angiography - What is MR Angiography?
- Magnetic resonance imaging (MRI) is a method of producing extremely detailed pictures of body tissues and organs without the need for x-rays.
- The electromagnetic energy that is released when exposing a patient to radio waves in a strong magnetic field is measured and analyzed by a computer, which forms two- or three-dimensional images that may be viewed on a TV monitor.
- MR angiography (MRA) is an MRI study of the blood vessels. It utilizes MRI technology to detect, diagnose and aid the treatment of heart disorders, stroke, and blood vessel diseases.
- MRA provides detailed images of blood vessels without using any contrast material. The procedure is painless, and the magnetic field is not known to cause tissue damage of any kind.
What are some common uses of the MRA procedure?
- Many patients with arterial disease now have it treated in the radiology department rather than undergoing surgery in an operating room.
- MRA is a very useful way of finding problems with blood vessels (blockages, blow-outs or abnormal connections) and determining how to best to treat those problems.
- The carotid arteries in the neck that conduct blood to the brain are a common site of atherosclerosis, which may severely narrow or block off an artery, reducing blood flow to the brain and even causing a stroke.
- If an ultrasound study shows that such disease is present, many surgeons now will do the necessary operation after confirmation by MRA, dispensing with the need for catheter angiography.
- MRA has found wide use in checking patients for diseased arteries in the head, so that only those with positive findings will need to have a more invasive catheter study.
- MRA also is used to detect disease in the aorta and in blood vessels supplying the kidneys, lungs and legs. Patients with a family history of arterial aneurysm (a ballooning out of a segment of the vessel wall) can be screened by MRA to see if they have a similar disorder that has not produced symptoms. If an aneurysm is found, it may be treated either by surgery or endovascular therapy, potentially avoiding serious or fatal bleeding due to rupture of the aneurysm.
What does the MRI equipment look like?
- The traditional MRI unit is a large tube surrounded by a circular magnet, in which the patient lies without moving for several seconds at a time.
- The patient is placed on a wheeled bed that is moved into the magnet.
- In recent years patient-friendly units have been designed, and examination in such units is becoming increasingly available. These machines are both shorter and wider than a conventional MRI unit, and do not fully enclose the patient.
- Some of the newer C-shaped units are even open on all sides, and so are very attractive to patients who tend toward claustrophobia.
How does the procedure work?
- Exposing the patient to radio waves in a strong magnetic field generates data that are used by a computer to create images of tissue slices.
- The magnetic field lines up atomic particles in the tissues called protons, which are then spun by a beam of radio waves and produce signals that are picked up by a receiver in the scanner.
- It is these signals that are processed by the computer to produce images. The resulting images are very sharp and detailed, and so are able to detect tiny changes from the normal pattern that are caused by disease or injury.
- Special settings are used to image various structures, such as arteries in the case of MRA.
How is the procedure performed?
- The patient is placed on a special table and positioned inside the opening of the MRI unit.
- A typical exam consists of two to six imaging sequences, each taking two to 15 minutes.
- Each sequence provides a specific image orientation and a specified degree of image clarity or contrast.
- Depending on the type of exam being done, the total time needed can range from 10 to 60 minutes, not counting the time needed to change clothing, have an IV put in and answer questions.
- When contrast material is needed, it is given by IV injection during one of the imaging sequences. It highlights blood vessels, making them stand out from surrounding tissues.
- The radiologist and technologist leave the examining room during the actual imaging process, but the patient can communicate with them at any time using an intercom.
- Some centers permit a friend to stay nearby, or a parent if a child is being examined.
- When the exam is completed the patient will be asked to wait to make sure that more images are not needed.
- The images will be reviewed by the radiologist, a medical doctor specially training in MRI, to prepare a diagnosis, which will be reported and forwarded to the referring physician.
What will I experience during the MRA procedure?
- The technologist will make you as comfortable as possible, but at times the receiver or the magnet may be within a few inches of your face.
- For those who become very uncomfortable when enclosed in a small space, a mild sedative is nearly always effective.
- With certain sequences, you may notice a warm feeling in the area being studied. This is normal, but do not hesitate to report it if it bothers you.
- If you receive a contrast material injection there may be some local coolness at the IV site. The loud tapping, buzzing or knocking noises that are heard during the exam can be quite loud.
- This may disturb some patients; all patients are provided with earplugs to reduce these sounds and protect your hearing.
Who interprets the results and how do I get them?
- A radiologist experienced in MRI will analyze the results and send a report to your physician, along with an interpretation of the findings.
- Your physician in turn will discuss the MRA findings with you.
- Some centers now send diagnostic reports and images over the Internet, speeding up the process.
What are the benefits vs. risks?
Benefits
- Detailed images of blood vessels and blood flow are obtained without having to insert a catheter directly into the area of interest, so that there is no risk of damaging an artery, or, in the case of the brain, causing a stroke.
- The procedure itself is shorter than after a traditional catheter angiogram. As well, there is no recovery time with the procedure, unlike the 4 to 6 hours needed for catheter angiography.
- MRA is less costly than catheter angiography.
- There is no exposure to x-rays during an MRI study.
- Contrast material may be injected to produce high-detail MR angiograms. The risk of an allergic reaction from MRA contrast is extremely low and kidney damage does not occur. This is different from catheter angiography or CT angiography, which make use of iodine-based contrast material, which has a much higher (though still small – less than 1 in 1,000) chance of some form of allergic reaction. In patients with kidney failure or poor kidney function, the iodine-containing contrast agents can worsen kidney function. Even without using contrast material, MRA can provide high-quality images of many blood vessels, making it very useful for patients prone to allergic reactions.
- As with catheter-based angiography or CT angiography, it may be possible to defer or cancel proposed surgery after getting the results of an MRA study. If surgery remains necessary based on the MRA, it can potentially be performed more accurately.
Risks
- There are no definite side effects from any type of MRI study, including MR angiography.
- Claustrophobia may be a problem, however. When it is severe and not relieved by giving a sedative, an alternative imaging method may have to be tried.
- If a metal implant is present but goes undetected, it may be affected by the strong magnetic field to which the patient is exposed. In addition, if the implant is close to the artery being examined it may be hard to get high-quality images.
- MRI generally is avoided during the first three months of pregnancy. Ultrasound is preferred at this time unless the woman might have a very serious condition that is best detected by MRA.
- If there are any effects of MRI on the fetus, none have been found as yet.
- The general rule for MRI and other diagnostic studies in pregnancy is that they should be avoided unless there is substantial risk from missing the correct diagnosis because the procedure is not done.
- Women who are breast-feeding should inform the radiologist and ask how to proceed. They may pump breast milk before the exam for use until the gadolinium contrast material has cleared from the body.
What are the limitations of MR Angiography?
- MRA does not image calcium, X-ray and CT angiography do see calcium on the images.
- The procedure has to be avoided in any patient having a pacemaker, some types of aneurysm clip (older types contain large amounts of iron, which is magnetic), some types of implanted neurostimulator, metallic ear implant, or metallic object within the eyeball.
- It should also be avoided if there is a bullet fragment near or in the brain, heart or spinal cord. It may also be avoided if the patient has a port for delivering insulin or chemotherapy.
- For patients who are very claustrophobic, adequate nursing or medical staff must be on hand to monitor sedation.
- The high-detail artery capability of MRA images does not yet match that obtained by x-ray catheter angiography. In particular, MRI of very small vessels may not be adequate for diagnosis and treatment planning, and regular catheter angiography will be needed.
- Occasionally it may be difficult to separate images of arteries from veins by MRA.


